Let us re-imagine senior rounds for the 21st century.
What I am about to describe does not require any new technologies or biomedical insights; it requires merely a different use of existing resources, different emphases in training and a national focus on the real-time use of clinical data as the evidentiary basis for clinical decision-making.
Senior rounds, in which the department chair meets with the senior residents to review the cases and processes of the prior day, are a decades-old tradition in medicine, and a valuable one. But as currently practiced in most residency programs, each senior resident reporting from their written notes or electronic health record system, the rounds fall far short of what they could be. Here, I offer an “alternative reality” for senior rounds, in hopes of catalyzing a discussion about why it is not the standard of care today. As the citations attest, the findings and techniques described here are all already available. So what are the principal obstacles then to the realization of this scenario?
Soma looked around the table, picking out the Seniors whom he would ask to give reports. He glanced at the screen to the side of the conference table listing the admissions and discharges of the prior day, wait times in the emergency department, diagnoses, and laboratory work ups.
He turned to Charles. “I see you admitted a 2-month-old for ‘rule-out’ meningitis but those laboratory results don’t look particularly worrisome.” Charles nodded but directed his tablet to throw up a local map with 5 red “X”s on the room’s screen1.
“I thought so too,” Charles said, “but the intern pointed out to me the 5 cases of N. meningitis detected in the last week by the State Department of Public Health, including one case in the same day-care center as this infant, so we thought it was prudent. We’re going to wait for culture results.” 2
Soma grunted non-committedly and moved on to Dolores: “I heard you had a little argument with the diabetes service over the discharge of Mr. Smith. Care to share what happened?”
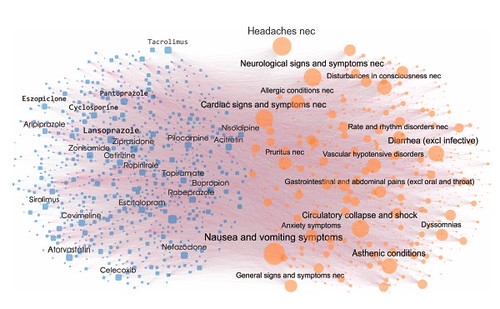
Dolores gave him a quizzical look for this ‘softball.’ “Yes, they were quite emphatic about switching Mr. Smith to a different oral hypoglycemic agent. I argued that its safety profile was far from as well established as the generics in the same structural drug class, and shared several publications with them that made the same point. But it’s only when I showed them that the risk for myocardial infarction, over the last four years, at our hospital was 50% higher for that drug as compared to others that they relented,” 3.
Soma looked at the curve of the myocardial infarction incidence of the drug in question, portrayed in red, and the six green lines showing the myocardial infarction incidence in the same hospital for the other oral hypoglycemic agents. The red curve rose above the green curves, well beyond the reach of their error bars.
He surveyed the seniors and returned to Dolores with a conspiratorial raised eyebrow. “You might want to share with the diabetes service that the FDA just reviewed these data and 20 data sets like it from other academic health centers. They all pointed in the same direction, and when they then reviewed the post-marketing data from the pharmaceutical company manufacturing the drug, the same trend was apparent. Chalk one up for evidence-based medicine. Speaking of which, Harvey, Mrs. Jones’ s headache ended up looking like a glioma on imaging. What are you telling her and her primary care provider about prognosis?”
Harvey directed the screen to replace the map with three graphs. “We’re scheduling the biopsy but it does look like Glioblastoma Multiforme (GBM), less than 2 cm in its largest dimension. The graph on the right shows the outcomes obtained at this hospital over the last 15 years for patients presenting with headaches not attributable to mass effect, like Mrs. Jones. The graph in the middle shows the other patients with GBM at this hospital without this ‘incidental’ presentation. The graph on the right suggests a better outcome but this might be due to the location of these incidental tumors. 4Regardless, it’s a tough prognosis but I shared this perspective with Mrs. Jones and her doctor. By the way, for reference you can see the national outcomes on the leftmost graph and you can see that ours are on average about 20% better as measured by survival times.”
Soma shared the slightest of winks and gestured towards Virginia.
“What about the infant you had discharged from the newborn service a week ago? I see that she was readmitted last night.” Virginia, looked up from the muffin that she had been steadily deconstructing, “Yes, that was unfortunate but not completely unexpected. We had not found any cause for the earlier episode of ventricular tachycardia in the first day of life. Because the tachycardia resolved spontaneously within 20 minutes, we decided to observe for another 72 hours. As there was no recurrence and no structural anomalies of the heart on imaging, we discharged the infant with a follow-up appointment with cardiology for a month from now. The ventricular tachycardia event did trigger an automatic rule from our electronic health record system (EHR) 5,6 which recommended a genetic screen for mutations in the depolarizing sodium and/or calcium channels. We checked the genotyping results on readmission and they are positive for a mutation in a calcium channel—CaCNB2b7—that was found in over one hundred children with ventricular tachycardia as per the National Registry and in no control cases. And by the way, as per our EHR data warehouse this is the fifth case in the last decade in our hospital alone. Although we were able to convert the infant back to sinus rhythm within 10 minutes, the cardiology service is considering use of an implantable cardioverter-defibrillator because of the chanelopathy.”
Soma interjected “Wasn’t the QRS interval abnormal after the first episode?” Virginia flicked the ECG from the EHR view on her tablet to the conference room screen. “No, as you can see, it was not, and there are several similar reports from the literature.” She followed by displaying several PubMed abstracts describing cases of normal ECG in infants with a chanelopathy.
Soma, turned towards the Chief Resident, “Mary Lee, are we going to have enough beds to keep up with all the activity in the ED?”
This question was asked so often that Mary Lee had already displayed the current bed census, as well as the projected lengths of stay based on several morbidity indices and predictors, on the conference room’s screen. “We’re in good shape. Worst case scenario still gives us 32 free beds by noon today8,9. Even with seasonal adjustment for influenza 10 we have at least 8 free beds including 2 in the ICU by the time the evening shift ends. That’s within the 95% confidence interval.”
Charles was glancing repeatedly at the smartphone he kept mostly hidden under the conference table.
“Is there a problem?” Soma asked, girding himself to deliver his well-worn diatribe on the distractions of modern communications.
Charles, stood up, pointing at the smartphone “Actually, there is. The ventilation requirements for one of the preemies is trending higher and the attending pediatrician is suggesting a caffeine infusion but I don’t think it is warranted based on the data. I had better go and check in with the team to see if they are on top of it.” 11
Soma leaned back with a smile. “I should warn you against ‘dismissing long-established clinical opinions without understanding the basis for their existence’12. But go ahead, rounds are over.”
(Thanks to Carey Goldberg for very constructive comments)
1. Brownstein JS, Freifeld CC, Madoff LC. Digital disease detection--harnessing the Web for public health surveillance. N Engl J Med 2009;360:2153-5, 7.
2. Fine AM, Nizet V, Mandl KD. Improved diagnostic accuracy of group a streptococcal pharyngitis with use of real-time biosurveillance. Annals of internal medicine 2011;155:345-52.
3. Brownstein JS, Murphy SN, Goldfine AB, et al. Rapid identification of myocardial infarction risk associated with diabetes medications using electronic medical records. Diabetes Care 2010;33:526-31.
4. Potts MB, Smith JS, Molinaro AM, Berger MS. Natural history and surgical management of incidentally discovered low-grade gliomas. J Neurosurg 2011.
5. Ullman-Cullere MH, Mathew JP. Emerging landscape of genomics in the Electronic Health Record for personalized medicine. Human mutation 2011;32:512-6.
6. Overby CL, Tarczy-Hornoch P, Hoath JI, Kalet IJ, Veenstra DL. Feasibility of incorporating genomic knowledge into electronic medical records for pharmacogenomic clinical decision support. BMC bioinformatics 2010;11 Suppl 9:S10.
7. Kanter RJ, Pfeiffer R, Hu D, Barajas-Martinez H, Carboni MP, Antzelevitch C. Brugada-Like Syndrome in Infancy Presenting with Rapid Ventricular Tachycardia and Intraventricular Conduction Delay. In: Circulation; 2011.
8. Mackay M, Lee M. Choice of models for the analysis and forecasting of hospital beds. Health Care Manag Sci 2005;8:221-30.
9. Littig SJ, Isken MW. Short term hospital occupancy prediction. Health Care Manag Sci 2007;10:47-66.
10. Reis BY, Pagano M, Mandl KD. Using temporal context to improve biosurveillance. Proceedings of the National Academy of Sciences of the United States of America 2003;100:1961-5.
11. Larkin H. mHealth. Hosp Health Netw 2011;85:22-6, 2.
12. Weiss S, Hatcher RA. Tincture of digitalis and the infusion of therapeutics. JAMA 1921;76:508-13.